
Suicidal thoughts are often treated solely as symptoms to be eliminated or risks to be managed, yet this narrow focus can overlook their deeper meaning. Many people who experience suicidal thoughts are also carrying unresolved trauma, loss, or chronic emotional pain. This article explores what suicidal thoughts may be trying to tell us, reframing the desire for death not as a literal wish to die but as a signal that something in a person’s life, identity, or relationships has become unbearable or unsustainable. When these thoughts are approached with curiosity, compassion, and attention to meaning alongside safety, therapy can become a space where individuals feel understood rather than silenced, and where genuine change can begin.
If safety feels uncertain
If you or someone nearby may act on suicidal thoughts or cannot stay safe, call or text the 988 Suicide & Crisis Lifeline now, use 988 chat, call local emergency services, or go to the nearest emergency room. The National Institute of Mental Health warning signs can also help loved ones recognize when immediate support is needed.
Why Suicidal Thoughts Are So Often Misunderstood
For many people, the moment suicidal thoughts arise, fear takes over. Individuals may feel ashamed, frightened by their own minds, or convinced that something is deeply wrong with them. Friends and loved ones often react with panic, while professionals may quickly move into assessment and crisis management.
While safety is essential, fear-based responses can unintentionally shut down the very conversations people most need to have. When suicidal thoughts are treated only as emergencies or warning signs, individuals may learn that honesty leads to consequences rather than care. As a result, many people hide these thoughts, even as they continue to suffer internally.
This silence can be deeply isolating. Instead of feeling supported, individuals may feel reduced to a problem that needs to be fixed or controlled. Over time, this can reinforce the belief that their pain is unacceptable or too much for others to hear. GoodTherapy’s guide on talking and writing about suicide offers helpful language for approaching the subject with care.
Key insight: Safety matters, but people are often more willing to talk honestly about suicidal thoughts when their pain is met with steadiness instead of panic.
A Different Lens: Suicidal Thoughts as Communication
Many people who experience suicidal thoughts are not expressing a true desire to die. Rather, they are expressing a desire for their pain to end. This distinction matters.
Suicidal thoughts can serve as a form of communication when other ways of expressing distress feel unavailable or unsafe. They may emerge when someone feels trapped, overwhelmed, exhausted, or disconnected from meaning and connection. In this sense, suicidal thoughts are not evidence of weakness or failure but signs that something in a person’s internal or external world is asking for attention.
Seen through this lens, the question shifts from “How do we make these thoughts stop?” to “What are these thoughts trying to tell us?” This reframing does not minimize risk. It makes room for both suicide prevention and a more humane understanding of pain.
PainA desire for pain to stop+
Suicidal thoughts may point to emotional pain that has exceeded a person’s current capacity to carry it alone.
LossA grief that has not been witnessed+
When grief is minimized, delayed, or unsupported, suicidal thoughts can become one way the mind signals that something important still needs care.
TraumaA nervous system stuck in survival+
Trauma can leave the body scanning for danger and the mind searching for escape, even long after the original harm has passed.
SupportA need for agency, connection, and safety+
The presence of suicidal thoughts can be a signal that support needs to become more immediate, collaborative, and compassionate.
A meaning-focused question can sound like
What feels impossible to keep carrying? What has gone unheard for too long? What kind of support would make the next hour safer? What would make life feel one small degree more livable?
The Role of Trauma, Loss, and Chronic Emotional Pain
For many individuals, suicidal thoughts are closely tied to unresolved trauma or loss. Trauma can disrupt a person’s sense of safety, identity, and trust in others. Loss, whether sudden or prolonged, can leave emotional wounds that do not heal easily, especially when grief is minimized or unsupported.
Chronic emotional pain may develop when someone has spent years feeling unseen, unheard, or required to carry more than they are equipped to manage. Over time, this accumulation of pain can overwhelm the nervous system. The body and mind may enter a state of exhaustion, where continuing to endure feels impossible.
In these moments, suicidal thoughts may arise as an imagined escape from relentless suffering. This does not mean the person truly wants life to end. Often, it means they cannot see another way forward. The CDC’s suicide risk and protective factors note that relationship, community, health, and life circumstances can all shape risk and protection.
GoodTherapy’s article on how complex trauma changes a person offers additional context for understanding why long-term pain can affect safety, trust, and identity.

When Survival Takes Precedence Over Living
Some people experiencing suicidal thoughts have spent much of their lives in survival mode. They may appear highly functional, meeting responsibilities, caring for others, and seeming capable. Internally, however, they may feel numb, disconnected, or deeply lonely.
Survival mode can keep someone alive, but it does not necessarily make them feel alive. When life becomes reduced to endurance rather than meaning, suicidal thoughts may surface as a response to this inner deadening. They can reflect a longing for rest, relief, or an end to constant striving.
Understanding this context allows for a more compassionate response, one that recognizes how much strength it has taken to survive up to this point.
A More Helpful Pathway
Unbearable pain
Honest language
Safety support
Meaning and agency
The Limits of Risk-Only Approaches
Traditional approaches to suicidality understandably focus on risk assessment and prevention. These strategies save lives and are often necessary. However, when risk management becomes the sole focus, the deeper emotional story can be overlooked.
Checklists and assessments do not capture the full complexity of human suffering. They cannot fully explain why someone feels trapped, empty, or hopeless. When people sense that only certain answers are acceptable, they may disengage or minimize their experience.
This does not mean safety should be ignored. Rather, it suggests that safety and meaning must be held together. When individuals feel heard and understood, they are often more willing to engage honestly in conversations about safety and support. For loved ones, GoodTherapy’s suicide prevention guide outlines ways to respond with directness and care.
How Therapy Can Create Space for Meaning
Therapy has the potential to offer something many people experiencing suicidal thoughts have never had: a space where their pain is taken seriously rather than feared or dismissed.
In a meaning-oriented therapeutic approach, suicidal thoughts are explored gently and respectfully. Clients are invited to talk about what feels unbearable, what has been lost, and what feels impossible to change. Instead of rushing to solutions, therapy slows the process down, allowing understanding to emerge.
These conversations do not encourage harm. They honor the reality of suffering while opening pathways toward agency, connection, and hope. If you are considering therapy, GoodTherapy’s step-by-step guide on how to find the right therapist can help you think through fit, safety, and support.
Looking for support?
You can use GoodTherapy to search for a therapist who can help you talk through suicidal thoughts, trauma, grief, and emotional pain with care.
Rebuilding Trust After Difficult Therapy Experiences
Some individuals experiencing suicidal thoughts have previously sought help and felt misunderstood, dismissed, or even harmed. These experiences can make it difficult to trust therapy again. When someone has learned that vulnerability leads to invalidation or control, they may approach new therapeutic relationships with understandable caution.
Acknowledging this history matters. Therapy can be effective only when trust is built slowly and collaboratively. A respectful therapeutic process emphasizes transparency, choice, and pacing, allowing clients to remain active participants in their own care.
Over time, consistent attunement and honesty can help repair not only the relationship with therapy but also a person’s relationship with themselves.
Reclaiming Agency and Choice
One of the most important aspects of healing is the restoration of agency. Suicidal thoughts often arise when people feel powerless, trapped, or unable to influence their circumstances. Therapy can help individuals reconnect with choice, even when options feel limited.
Agency does not mean forcing positivity or making drastic changes overnight. It may begin with small acts of self-understanding, boundary setting, or self-compassion. As people begin to understand what their suicidal thoughts are communicating, they can explore new ways of responding to their needs.
This process often includes learning to recognize emotional and relational patterns, identify values and sources of meaning, develop healthier ways to ask for support, build tolerance for difficult emotions, and imagine change without overwhelming the nervous system.
When depression is part of the picture, it can be especially important to have timely support. GoodTherapy’s article on depression and suicide explains when to seek help and why warning signs should be taken seriously.
When Hope Feels Out of Reach
Hope is often misunderstood as optimism or certainty. For people experiencing suicidal thoughts, hope may feel distant or unrealistic. In therapy, hope does not need to be forced or manufactured.
Sometimes hope begins as a sense of being less alone. Sometimes it shows up as curiosity, or as a willingness to stay present for one more conversation. These small shifts matter.
Healing is rarely linear. There may be moments of progress alongside moments of discouragement. A supportive therapeutic relationship can help individuals stay connected through these fluctuations, offering steadiness rather than pressure.
A Compassionate Closing
If you or someone you love experiences suicidal thoughts, it is important to know that these thoughts are not a personal failure. They often reflect pain that has gone on too long without adequate support. They may be signaling unmet needs, unresolved grief, or a longing for change that feels out of reach.
Understanding what suicidal thoughts may be trying to tell us does not replace the importance of safety. It deepens it. When people feel understood rather than judged, they are more likely to reach out, stay engaged, and explore new ways of living.
Therapy can be a place where these conversations are held with care, respect, and honesty. When meaning and compassion are allowed alongside safety, the possibility of genuine and lasting change becomes more accessible.
If you are struggling or feeling unsafe, reaching out for support can be an important step. Speaking with a trusted person, a mental health professional, or a local crisis resource can help you navigate this moment with care and support. The NIMH 5 action steps can also help loved ones respond when someone is in emotional pain.
Frequently Asked Questions
Direct answers about suicidal thoughts, therapy, trauma, grief, and immediate support.
Take the Next Step
You do not have to make sense of suicidal thoughts alone. Compassionate support can help hold both immediate safety and the deeper meaning beneath the pain.
Find a Therapist Near You >
 |
About the Author Kristin RobertAssociate Marriage and Family Therapist Kristin Robert is an Associate Marriage and Family Therapist in Westlake Village, California. Her work centers on helping individuals and couples navigate intimacy, loss, betrayal trauma, grief, anxiety, relationship patterns, and major life transitions. Her GoodTherapy profile lists her work with teens, adults, and elders, and concerns including grief and loss, anxiety, depression, trauma, relationship pain, life transitions, and suicidal ideation and behavior. Her approach emphasizes compassion, honesty, meaning-making, and support for people navigating painful or uncertain seasons. |
 Over the past couple of months, there has been a teen suicide at each of two neighboring high schools in my community. To say this is tragic is an understatement. As a child and adolescent therapist, I knew these suicides were going to make their way into my therapy office during the weeks that followed. In fact, I was going to ensure they did because I am a firm believer it is important for therapists, and other adults, to talk with teens about suicide. Why? Because teens are already talking about it, and it is likely the people they are talking to are not knowledgeable about how to help them process such an act in a healthy and helpful way.
Over the past couple of months, there has been a teen suicide at each of two neighboring high schools in my community. To say this is tragic is an understatement. As a child and adolescent therapist, I knew these suicides were going to make their way into my therapy office during the weeks that followed. In fact, I was going to ensure they did because I am a firm believer it is important for therapists, and other adults, to talk with teens about suicide. Why? Because teens are already talking about it, and it is likely the people they are talking to are not knowledgeable about how to help them process such an act in a healthy and helpful way.
When a teen in a community commits suicide, there is a full spectrum of feelings among other teens. Teens may feel confused, sad, angry, curious, anxious, numb, or scared. Some may feel triggered and have their own thoughts about suicide or self-harm. Some may be frustrated by the sudden outpouring of love and attention that the teen who died gets, especially if it feels disingenuous. And some may have a hard time processing what would bring a peer to decide to end their life. Regardless, these reactions often bring a desire to talk about what happened. In seeking to understand, teens may turn to social media, including Instagram and Facebook pages that share unfiltered photos and information on suicide and self-harm. These are not places we want our children to be learning about such topics.
[fat_widget_right]
Talking with teens about suicide is also important because they are often the first line of defense in preventing teens from ending their lives. Most suicidal teens have expressed their suicidal ideation, whether blatantly or subtly, to friends or peers either in person or via social media. Unfortunately, many teens don’t know what to do with the information, are unsure of the signs to look out for, or don’t want to be “that person†who snitches or gets involved.
Especially following the suicide of an adolescent, there are things that adults can do to not only help teens process the loss but also help prevent other suicides. The first is to know and be able to recognize the signs and symptoms of depression and suicidal ideation. Following a suicide, these signs and symptoms may be heightened in adolescents, especially in already depressed, anxious, or suicidal teens:
- Depressed or anxious mood
- Frequent running away
- Expressions of suicidal thoughts and talk of death
- Withdrawal from friends, family, and activities
- Impulsive and sometimes aggressive behavior
- Alcohol and/or drug abuse
- Engaging in high-risk behaviors
- Social isolation
- Low self-esteem
- Giving away meaningful belongings
- Self-harm behavior
- Suggestive social media messages, videos, posts
Equally important is how to take action and be a safety net for adolescents in need. As an adult, it is important to be available to adolescents and talk openly with them about suicide. It is so important that adults check in directly with teens following the suicide of a peer, especially if there have been prior concerning signs or symptoms. Parents, teachers, and counselors alike should process the loss with teens and explore how they are feeling, what they are thinking, and how they are coping with the loss. Some helpful questions include:
It can feel scary to talk about suicide, but in my experience it is important to talk directly with adolescents to help them deal with this topic. If you are unsure how to talk with your teen about suicide, connect them with their guidance counselor or a therapist who can help them process any feelings they might be having.
- How well did you know the teen who died?
- How do you feel about the news?
- What are some thoughts or questions you have been having since hearing about it?
- Have you talked to anyone about the suicide?
- Have you seen any information online about suicide?
- How has your school (whether it is the school that the person who died attended or not) been addressing the suicide?
- Have you ever thought about killing or hurting yourself? What can you do or who can you talk to if you have those thoughts?
- Do you know anyone who has expressed those thoughts/feelings? How have you handled that? How do you feel about that?
- What can you do if you hear that someone has suicidal thoughts?
After exploring some of these questions, it is important to help them come up with a plan for what they can do if they have a concern for a peer and explore any potential resistance. It can be helpful to communicate that there are ways to report their concerns in a confidential way that can protect their relationship with the peer. Emphasize the importance of doing something.
It is also important to help them identify their own coping strategies to manage things such as anxiety, depression, peer problems, and stress, as well as to help them identify a trusted adult whom they can talk to if they are struggling. Let them know they are not alone.
It can feel scary to talk about suicide, but in my experience it is important to talk directly with adolescents to help them deal with this topic. If you are unsure how to talk with your teen about suicide, connect them with a therapist or guidance counselor who can help them process any feelings they might be having. Know you are not alone, either. Together, hopefully lives can be saved.
 13 Reasons Why is a runaway hit with teens and tweens. Here’s what you need to know and how to discuss the controversial topics it introduces (and doesn’t always handle responsibly) with your kids.
13 Reasons Why is a runaway hit with teens and tweens. Here’s what you need to know and how to discuss the controversial topics it introduces (and doesn’t always handle responsibly) with your kids.
Netflix’s 13 Reasons Why glamorizes suicide to a vulnerable audience. It sends the troublesome message that if you are not able to find your voice in life but are thoughtful about planning your death, you can bring about justice and have the last word from beyond.
What a way to stick it to the people who contributed to your decision to end your life.
[fat_widget_right]
The teen years are fraught with challenges. Unfortunately, bullying, sexual objectification, and unstable relationships are some of the issues adolescent girls often face. The show’s protagonist, Hannah Baker, experienced a series of heinous assaults—on her character and her body—at the hands of her peers.
Parents, classmates, and school faculty were not there for her, as she needed them to be. She handled her pain by ending her life at age 17. She was a bright girl with a dark sense of humor and unknown potential.
Instead of seeking help, she spent the last week of her life crafting an elaborate scavenger hunt as a legacy to teach the people who had hurt her a lesson. She channeled energy that could have saved her life into planning her death and the events that would follow.
I see teens in my private therapy practice. Many of them are watching this show, which makes suicide dangerously relatable and depicts it as a form of self-expression. I fear we are going to see a surge in teen suicidality.
Suicide is the second-leading cause of death among young people ages 15 to 24. More than 5,000 people in that age group die by suicide every year in the United States. Graphic depictions of suicide have been shown to exacerbate suicidal ideation in already troubled teens, particularly if the act is portrayed as imaginative and brave. Adolescents who think everyone paid attention to the pretty, misunderstood girl from 13 Reasons Why may be tempted to follow her lead.
The show shines a light on the damaging “butterfly effect†the self-serving actions of insecure high school students jockeying for social status can cause. It opens up an important conversation about “slut-shaming†and sexual assault. But it fails to let teens know suicide is not an appropriate response to tragic circumstances.
As it is, too many teens struggle with depression and suicidality made worse by the cruel politics of high school. This show gives them an out of sorts, painting suicide as an opportunity to be immortalized in death.
Her suffering makes her a heroine—maybe even a modern-day martyr. But is that really the message we want our kids to take away? That if they are clever enough about the way in which they plan their untimely death, they will make an impact in a way that would never have been possible if they had struggled through it and lived?
What does this show teach kids about the value of their lives?
Hannah Baker made audiotapes and began a chain, arranging to have them delivered to each person she holds responsible for contributing to her suicide. She declares each one guilty in a posthumous trial, shaming them among their peers and riddling them with fear of social, academic, and legal consequences if word gets out about what they did.
She lives on as a narrator, almost as if she is watching her classmates’ lives unravel in response to the information she disseminates among the group. She is the “star” of the show.
Teens need to understand if they end their lives, they are not going to be watching anything unfold, and they are not going to be the star of any show. That’s it. Game over. Pain over but also opportunity over. No witty voiceover or indie soundtrack. Life over. Once she decided to end her life, it seems Hannah took more pains to plan for events after her death than to seek a reason to live.
High school can be vicious. At this treacherous developmental stage, fitting in can seem like life and death. Kids betray friends to avoid humiliation, impress peers, and secure their place in the social hierarchy. Add to that the rapid changes occurring in the body and brain, the pressures of navigating dating and sexuality, worries about grades, extracurricular activities, college, and family issues, and it’s a perfect storm of stress.
Teens need to understand if they end their lives, they are not going to be watching anything unfold and they are not going to be the star of any show. That’s it. Game over. Pain over but also opportunity over. No witty voiceover or indie soundtrack. Life over.
But the answer is not to opt out. And this needs to be made clear to a population susceptible to self-doubt and impulsivity. Adolescents’ developing brains cannot fully grasp the impact of their actions, rendering them prone to ill-conceived decisions.
Most choices can be remedied and may serve as valuable lessons. But utilizing one’s suicide as an intricate revenge fantasy? Teens need to recognize this irreversible act will not bring the satisfaction they imagine. Despite her voiceover implying otherwise, Hannah Baker did not live to see the impact of her tapes.
The teen years can be agonizing. One out of six high school students seriously considers suicide. The message needs to be made clear. Once you take your life, there is no coming back. There is no chance to use your pain to create something beautiful, to use your empathy to offer people friendship or hope, or to triumph over those insecure, self-important kids who stepped on you to prop themselves up.
There is no realizing they cross your mind less and less as you find contentment, fulfillment, and connection with people who are not fixated on their own image, or that there are no more cool kids—life after high school is about finding your passions and people who uplift you.
With many teens viewing media on their personal devices, it is challenging to stay on top of what your kids are seeing, but it’s important to know what is influencing them. None of the teens’ parents in the show have a real sense of what is going on in their lives while they make savage, illegal, and, in Hannah’s case, fatal decisions.
Teens don’t tell their parents everything. It’s stage-appropriate for them to reject their parents’ ideas and carve out their own identities, but you have a responsibility to engage with your kids and know their friends. Encourage them to share their goals and setbacks with you.
Pay attention.
There are clues when something is wrong, but you have to look for them. How are their grades? What do they do with their free time? Which activities are they involved in? What are their interests? How is their mood? Who are their friends?
13 Reasons Why raises a lot of serious issues worth discussing, but it dangerously romanticizes suicide and elevates it to a heroic act. Though Netflix does not release ratings data, it is the most-tweeted-about television show of 2017, making it clear this is a cultural phenomenon.
Since your kids may have watched it already, use it to talk to them about bullying, depression, feelings of isolation, and suicidality. Ask them what they think about choosing to end one’s life and what they would do if they felt hopeless. Offer them counseling, whether it’s the guidance counselor at school, a community counseling center, a private practice therapist, or a teen group.
Frame it as a resource to be utilized when they struggle and remind them they can come to you, no matter how concerned they may be about your reaction. Let them know you love them unconditionally and are there to help in any way you can. Ask how they are doing if they appear to be hurting. They may not share with you because they think you aren’t interested or you’ll criticize or worry.
Create a climate that lets them know you care and want to support them without passing judgment or trying to live their lives for them. Talk to your kids and let them know it gets better and help is available.
Sometimes the most difficult choice is to struggle on, but all emotions are time-limited. Just as there were joyful moments in the past, there will again be moments that make life worthwhile. Hardships provide us contrast with which to appreciate them and with the tools to grow resilient.
If you are feeling suicidal, or know someone in crisis, please reach out for help. The 988 Suicide & Crisis Lifeline is 988.
References:
- Gould, M. S., & Lake, A. M. (2013, February 6). The contagion of suicidal behavior. Contagion of violence: Workshop summary. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK207262
- Holmes, L. (2017, July 18). Netflix shows are sparking conversation about mental health. But is it helping? Huffpost. Retrieved from http://www.huffingtonpost.com/entry/netflix-mental-health_us_5968f080e4b03389bb16f500?utm_content=buffereed8d&utm_medium=social&utm_source=twitter.com&utm_campaign=buffer
- Koebler, J. (2013, May 21). Study: Suicidal thoughts are ‘contagious’ in teens. U.S. News. Retrieved from https://www.usnews.com/news/articles/2013/05/21/study-suicidal-thoughts-are-contagious-in-teens
- Statistics about youth suicide. (n.d.). Youth suicide prevention program. Retrieved from https://yspp.org/about_suicide/statistics.htm
- Stoek, A. V., McCauley, E., Flynn, C., & Stone, A. (2010, December 1). Thoughts of death and suicide in early adolescence. Suicide and life-threatening behavior. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2819538
 In 2017, the suicide rate reached a 33-year high. Suicide is now the second-leading cause of death among teenagers, and an American dies by suicide every 12.8 minutes.
In 2017, the suicide rate reached a 33-year high. Suicide is now the second-leading cause of death among teenagers, and an American dies by suicide every 12.8 minutes.
Deaths by suicide are often surrounded by unanswered questions. Those left behind may feel a combination of grief, guilt, anger, and confusion. People experiencing suicidal thoughts often struggle to feel heard. Myths about suicide, such as the idea that talking to a suicidal person can make them more suicidal, are pervasive.
Suicide is a preventable tragedy. Knowing what to say and what to do when someone is having thoughts of suicide can save lives. The way we talk about suicide matters, and the effects of these discussions extend far beyond conversations with loved ones. Research suggests the way journalists write about suicide can increase the suicide rate. A constructive approach to reporting on and talking about suicide raises awareness and cultivates empathy without sensationalizing death.
Why We Need to Talk About Suicide
“One of the biggest misconceptions around suicide is that talking about it will cause it,†said Lisa Danylchuk, LMFT. Danylchuk is an Oakland, California, therapist who specializes in treating trauma survivors. She often works with people experiencing suicidal thoughts.
[fat_widget_right]People who talk about suicide are not doing it to get attention. Bringing up suicide can be very difficult, so if someone broaches the topic of suicide, it suggests they want help. Suicide is rarely impulsive, and many people who die by suicide first discussed it with a loved one.
People concerned about a loved one’s emotions should consider broaching the topic of suicide. Initiating a discussion does not implant the idea. Instead, it can provide a safe space to talk about stigmatized feelings.
“Giving people a space to explore their feelings related to suicide often helps them process their feelings,†Danylchuk said. “It also helps those concerned to monitor the severity of suicidal ideation and reach out for the appropriate support when necessary.â€
The American Foundation for Suicide Prevention (AFSP) offers a basic primer on the benefits of talking about suicide. Talk Saves Lives organizes brief presentations in communities across the nation to help people recognize the warning signs of suicide and learn how it can be prevented.
Reporting on Suicide: The Contagion Effect
Talking about suicide does not cause suicide, but reporting on it might. Articles and stories about suicide can create a contagion effect, potentially pushing people who are already at risk of suicide to more seriously consider it. Suicide prevention experts call this the Werther Effect, named for the novel The Sorrows of Young Werther by Johann Wolfgang von Goethe. After the 18th century publication of the novel, young men began imitating its protagonist. Some copied his suicide and suicide method. Some areas banned the novel in an attempt to save lives.
Researchers have observed a contagion effect associated with glamorized and heavily publicized suicide ever since.
“We have more than 100 studies from around the world now that demonstrate how media reports on suicide impact the risk of contagion,†said Daniel Reidenberg, PsyD, the executive director of Suicide Awareness Voices of Education (SAVE). “The more frequently a story is reported on, the placement of the story in a newscast or in print, the more graphic and sensational a story—all impact the audience. We know that when suicide is romanticized or glorified, that too leads to suicide contagion. When someone is memorialized in the media, some believe they too will be just like the person they are seeing in the news, and that gives them an identity or recognition that they don’t necessarily feel.â€
Reidenberg trains journalists who report on suicide, and he helped develop a list of best practices for journalists reporting on suicide. He says most journalists do not understand their role in contagion, yet simple changes in the way journalists talk about suicide can make a big difference. A 2007 study of Austrian guidelines for reporting on suicide found use of the guidelines lowered the nation’s suicide rate by 80% in just six months.
Guidelines for Reporting on Suicide
Reidenberg says media outlets tend to rely on stereotypes and clichés when reporting on suicide, but he cautions that suicide is never because of a breakup or a bad grade in school. Multiple factors figure into the decision for someone to take their own life. Reports that gloss over this nuance make it seem like a single bad event is enough to lead to suicide.
Likewise, reports that focus only on positive characteristics of the person who died can glamorize suicide. People who feel hopeless might think they will be remembered in the same way. The same is true for reports that highlight loved ones’ reactions.
Experts make the following recommendations to journalists reporting on suicide:
- Avoid sensationalized headlines that focus on suicide or the method of death. Report the facts instead, and avoid using suicide as an attention-grabbing topic.
- Use neutral photos, such as school pictures, rather than images of bereaved family.
- Include contact information for a suicide hotline.
- Avoid hyperbolic language such as “suicide epidemic.†Use specific language such as “rise in the suicide rate.â€
- Don’t use “successful†to refer to a completed suicide.
- Don’t characterize a suicide as sudden or without warning, and don’t focus on a single precipitating factor, such as a job loss. Instead, include a list of warning signs and intervention tactics.
- Don’t highlight or provide excerpts from a suicide note.
- Don’t treat suicide as criminal or report on it in a manner similar to criminal acts. Focus on suicide as a public health concern.
- Don’t interview or quote police or first responders. Instead, ask suicide prevention or mental health experts for insight.
- Don’t describe the method of suicide, particularly not in graphic detail.
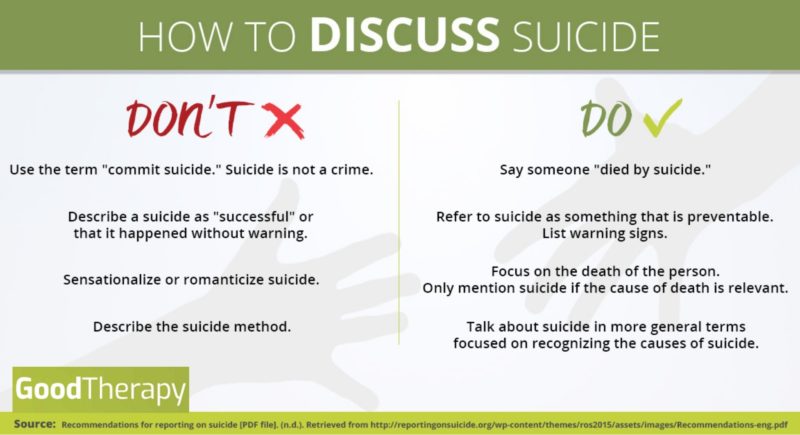
These guidelines reduce the likelihood that vulnerable people will see suicide as thrilling, glamorous, or the inevitable result of a sudden difficulty. They also help reporters avoid victim blaming and reduce stigma by treating suicide as a health concern, not a moral or criminal issue.
How to Talk to a Suicidal Person
“We know that it is okay to talk about suicide, even with someone who might be thinking about it,†Reidenberg said. “Doing so does not make them want to die more or lead them to attempt suicide. In fact, talking with someone who is thinking about this can reduce their level of anxiety, distress, and hopelessness and encourage them to seek help. Research shows that if you’re worried about someone, talk to them. It’s okay to do that.â€
Danylchuk echoed these sentiments, suggesting a simple aphorism: “When in doubt, talk it out.â€
Yet, talking to a suicidal person can be intimidating. Together Strong, an organization and app that helps veterans adjust to civilian life after deployment, suggests beginning the conversation directly, without judgment. Make an observation about recent behavior, or ask an open-ended question about how the person is feeling.
Don’t talk about how the person is making you feel, and don’t judge their behavior. This shuts down conversation, and can increase feelings of frustration and hopelessness. “You’re stressing me out with your negativity†is unhelpful. “I’ve noticed you seem sad lately. How are you feeling?†is more effective.
When a person shares their feelings of hopelessness or thoughts of suicide, try the following strategies:
- Validate their feelings. It may be tempting to minimize their suffering in an attempt to get them to change their suicidal thoughts. Validation, however, can help your loved one feel understood. It encourages them to keep talking. Talking can save lives.
- Don’t act shocked, angry, or disappointed. It can be difficult to talk about suicide, and these reactions shut down the discussion.
- Listen attentively, and avoid rushing your loved one or appearing annoyed.
- Know that people contemplating suicide often have mental health issues. Your loved one might say things that don’t make sense or that you dislike. Avoid judging or labeling them.
- Take talk of suicide seriously. Never suggest a person take their life in a moment of your own exasperation. Never suggest they are only seeking attention.
- Allow your loved one to freely express their emotions in a way that works for them. Don’t judge or shame them for using profanity, questioning deeply held spiritual beliefs, expressing anger at loved ones, or saying something that shocks you.
- Ask the person if there is something they need or something you can do to help. This allows them to ask for something—a ride to the emergency room or companionship, for example—if they need it. Be prepared for them to say no or that they don’t know, but don’t end the conversation there.
- Ask your loved one if they can think of reasons to live. Devising a list of reasons to live can reduce the power of suicidal feelings. If your loved one is unable to devise such a list, don’t judge, argue with, or shame them.
Preventing Suicide
When someone expresses suicidal thoughts or feelings, remaining engaged in a conversation is a powerful antidote. People who are able to talk have an outlet for their pain. Companionship and conversation can be temporary antidotes to thoughts of suicide.
To further reduce the risk:
- Do not leave a person experiencing suicidal thoughts alone. If you can’t be with them, find someone who can, such as a parent, a friend, or other loved one.
- Call a suicide hotline. The person on the other end of the line can connect you to emergency intervention services in your area, offer you the support you need to be a good listener, and answer questions about suicide. The 988 Suicide & Crisis Lifeline offers an online chat, or you can call 988 for help over the phone.
- Don’t agree to keep someone’s thoughts of suicide secret, but don’t use a person’s feelings to humiliate them. Share their feelings with someone who is equipped to help. That person might be a parent, sibling, or loved one. It could also be a mental health expert. The right person varies. For example, a teacher worried about a suicidal teenager with abusive parents should consider talking to someone other than the teen’s parents.
- Remove objects the person could use to hurt themselves, such as drugs or weapons.
- Ask the person if they can agree not to kill themselves for a short period of time. Encourage them to give it a day, a week, or even an hour. This can be particularly helpful if you cannot be in physical contact with the person or if they are waiting to receive mental health care.
- Encourage the person to go to the emergency room or to a crisis mental health facility. If you can, offer to go with them so they feel less alone.
- Contact an emergency service. Call 911 or an ambulance if you believe the person is in immediate danger or if they have already attempted suicide. In some regions, the police have suicide intervention training. In other regions, mobile mental health crisis services are available. Researching options ahead of time can help you know what number to call.
- Contact your local chapter of the National Alliance on Mental Illness (NAMI). NAMI provides resources and support to people who love someone who is experiencing mental health issues.
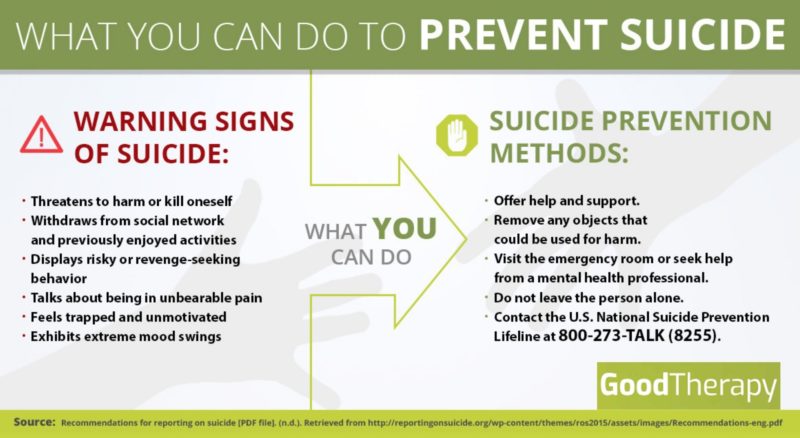
Suicide Warning Signs
While some people experiencing suicidal thoughts may openly share these thoughts, others may suffer in silence. The AFSP highlights the following warning signs:
- Talk of feeling trapped, being a burden, having no reason to live, or facing unbearable pain
- Changes in mood, including increases in anxiety, depression, anger, loss of interest in life, or feelings of shame and humiliation
- Reckless behavior, including aggression or increased use of drugs or alcohol
- Giving things away
- Isolating oneself from loved ones, or reaching out to people to say goodbye
Mental health issues such as depression and anxiety are significant risk factors for suicide. People who express suicidal feelings who have access to a weapon, or who have a clear plan or suicide method, are at a heightened risk. Some other risk factors for suicide include:
- Experiencing a stressful life event, though no single factor causes suicide
- Experiencing prolonged stress, such as bullying or a chronic illness
- Exposure to another person’s suicide, such as the suicide of a classmate, or to sensationalized reports of suicide
- Previous suicide attempt
- A family history of suicide
Suicide is preventable, and bystanders can help. If you need help for yourself or someone you love, you can call the following phone numbers for help:
- 988 Suicide & Crisis Lifeline: 988
- NAMI HelpLine: 1-800-950-6264
- Trans Lifeline: 1-877-565-8860
- National Center for Posttraumatic Stress Disorder Veterans Crisis Line: 988, ext. 1
- Mental Health America (for area-specific referrals): 1-800-969-6642
- Postpartum Support International (for general information, not crisis intervention): 1-800-994-4773
- National Sexual Assault Hotline: 1-800-656-4673
References:
- Increase in suicide in the United States, 1999-2014. (2016, April 22). Retrieved from https://www.cdc.gov/nchs/products/databriefs/db241.htm
- Kirkwood, A. (n.d.). Tips for talking to students about suicide [PDF]. Oregon Youth Suicide Prevention Campaign.
- Niederkrotenthaler, T., Herberth, A., & Sonneck, G. (n.d.). The ‘Werther-effect’: Legend or reality? Neuropsychiatry, 21(4), 284-290.
- Suicide: 2016 facts and figures [PDF]. (2016). American Foundation for Suicide Prevention.
- Suicide claims more lives than war, murder, and natural disasters combined. (n.d.). American Foundation for Suicide Prevention. Retrieved from https://afsp.donordrive.com/index.cfm?fuseaction=cms.page&id=1226&eventGroupID=9AA19459-C880-0E26-61312B15147B2E0A&cmsContentSetID=D5C4DC12-C299-258B-B0B6FCF9EF015CE0
- Suicide prevention: Myth or fact? (n.d.). Retrieved from http://ucc.nd.edu/self-help/depression-suicide/suicide-prevention-myth-or-fact/
- Suicide statistics. (n.d.). American Foundation for Suicide Prevention. Retrieved from https://afsp.org/about-suicide/suicide-statistics
- Tips and tactics: Recognizing red flags [PDF]. (2014). Together Strong.
- VanOrman, A., & Jarosz, B. (2016, June). Suicide replaces homicide as second-leading cause of death among U.S. teenagers. Retrieved from http://www.prb.org/Publications/Articles/2016/suicide-replaces-homicide-second-leading-cause-death-among-us-teens.aspx
 Amy Bleuel, the mental health advocate who founded global nonprofit Project Semicolon, died at age 31 last month. The cause of death was suicide.
Amy Bleuel, the mental health advocate who founded global nonprofit Project Semicolon, died at age 31 last month. The cause of death was suicide.
Amy Bleuel and Project Semicolon
Bleuel founded Project Semicolon in 2013 to honor her father, who died by suicide. The project uses a semicolon to symbolize remaining alive through difficult times. Just as a semicolon denotes a pause in—rather than an end to—a sentence, the semicolon symbolizes moving forward rather than stopping. Many people who embrace the semicolon symbol say they see their lives as unfinished stories.
The semicolon quickly caught on as an international symbol of hope. Semicolon tattoos and art became a way to signal triumph in the face of suicidal thoughts and mental health issues.
Bleuel experienced mental health issues, including depression, for two decades. According to the Project Semicolon website, she also dealt with bullying, rape, self-harm, and mental health stigma.
Project Semicolon actively solicits stories of hope and triumph to encourage people who have faced similar obstacles to persist, seek help, and support one another.
Suicide as a Public Health Issue
[fat_widget_right]Suicide rates climbed to a 30-year high in 2014. Suicide is the 10th leading cause of death nationwide and the leading cause of death among people ages 10-24. While a variety of factors often contribute to suicide, many people who die by suicide meet diagnostic criteria for at least one mental health condition.
Men are significantly more likely than women to die by suicide. Middle-aged men experienced a 42% increase in suicide between 1999 and 2014.
Suicide is preventable, and Project Semicolon advises people to notice warning signs and take suicide threats seriously. For help, contact the 988 Suicide & Crisis Lifeline at 988. The Lifeline also offers a live chat feature here.
To support Project Semicolon, get help, or share your story, visit the Project Semicolon website.
References:
- Curtin, S., MA, Warner, M., PhD, & Hedegaard, H., MD, MSPH. (2016, April 22). Increase in suicide in the United States, 1999-2014. Retrieved from http://www.cdc.gov/nchs/products/databriefs/db241.htm
- Facts about mental illness and suicide. (n.d.). Retrieved from http://depts.washington.edu/mhreport/facts_suicide.php
- Obituary for Amy Bleuel. (2017, March 24). Retrieved from http://www.pfotenhauerfuneralhome.com/m/?p=memorial&id=1943951
- Our founder. (n.d.). Retrieved from https://projectsemicolon.com/our-founder/
- Suicide prevention. (n.d.). Retrieved from https://projectsemicolon.com/suicide-prevention/
 I hardly dare to write or even think about suicide, a topic difficult enough to discuss when it is not outright painful. Suicide, attempted or completed, has touched the lives of many. You may know someone who has died by suicide or someone who has made an attempt. You may have experienced thoughts of suicide yourself.
I hardly dare to write or even think about suicide, a topic difficult enough to discuss when it is not outright painful. Suicide, attempted or completed, has touched the lives of many. You may know someone who has died by suicide or someone who has made an attempt. You may have experienced thoughts of suicide yourself.
There are people who consider the act of suicide to be a sin, an act tantamount to murder, and consider it unforgivable under any circumstances. My personal belief, though, is that some situations, such as long-term physical pain or terminal illness, may make suicide seem like a rational course of action. Of course, emotional pain can be intolerable too. Severe depression, for example, which may feel endless and can be a match for tormenting physical pain, can often play a part in the development of suicidal thoughts.
When someone we love dies by suicide, whatever the reason behind their choice, we are likely to feel unspeakable grief. We may feel angry or hurt; we may perhaps experience guilt. Along with these emotions, we might feel a desire for answers and explanations. We want to know why this happened, how it could have happened.
When A Loved One Dies By Suicide
People who complete suicide sometimes leave notes or discuss their plans with loved ones. Other people might say nothing. Even when we have some knowledge or understanding of a person’s reasons, suicide leaves us ungrounded. We need something to hold onto.
I myself know people who have died by suicide. My father’s cousin, who was fatally ill, asked to be removed from his respirator so he could die on his own terms. Another of my cousins who was incurably ill and in pain did something similar. They both said goodbye to close family members before passing on.
One lovely young man I knew who was battling addiction also chose to end his life. He was extraordinarily kind, funny and smart—a feeling soul. Before he died, he took his mother on a trip to the northwestern United States, a place they had both wanted to visit. I don’t know if they discussed his plans, but I do believe this was his way to say goodbye and tell her he loved her. I do feel he was, in some way, looking to be close to her and compensate, in a way, for his death. [fat_widget_left]
Some months after this young man’s death, I read a Facebook post from an older woman, a message that was unusually warm. Her wishes to her friends and her thoughts about life were so lovely—it took time and rereading to realize it had been a goodbye to those of us reading, a suicide note—that, in fact, she had already passed on by the time I read the post. Many of us wrote back, remembering her gifts and her compassion, expressing their love. I was not the only person who couldn’t believe she was dead.
A colleague with an incurable disease planned her suicide very carefully. She wanted to make sure she would succeed. She wanted to protect her husband and children. She wanted to live as long and as well as she could, and then she wanted to die.
Again, I hesitate to write about suicide. My intention is not to inflict pain, to challenge anyone’s beliefs, or to cause difficult feelings. I only want to help those left behind, the survivors, survive, but I’m not sure if I can.
The people I’ve written about just now had deep relationships with others. They took care of the people around them, both in their lives and in their deaths. Each of these people understood what they were doing and knew their choice would have an impact on the people close to them.
They said goodbye, either directly or metaphorically, to make sure those who survived them knew they were loved. And though their absence left a painful, unreal space, a hole, they are all still alive inside of me. There are always reminders that they are gone, as there should be. They were here, but now they are physically not, though they live in memories and as part of our emotions.
Some might consider love and suicide to be antithetical. But I believe death and love are both so big that they encompass their meanings and their opposites, their synonyms and their antonyms.
To me, the most touching death of all was that of the young man who traveled with his mother before he died. The enormity of his love, and of all that he left behind, is almost more than I can bear. I find his death so poignant because he was young—not yet thirty—and because he and his mother embodied the primal pair of mother and child. Birth and love. Ultimate connection, followed by the ultimate disconnection. But not. (The iconic image of the Pieta—the Virgin Mary holding the body of the dead Christ in her lap, appears before my eyes as I write this.)
When your life has been touched by suicide, working through the complicated feelings that develop can be a challenging process. The support of a qualified therapist or counselor can often be of benefit. If you are having thoughts of suicide, we urge you to reach out. The 988 Suicide & Crisis Lifeline (988) is available at any time, day or night. Additional crisis information and resources are available here.
If you would like to read further on this topic, I suggest Linda Phillips’ book A Beautiful Here: Emerging from the Overwhelming Darkness of My Son’s Suicide. [amazon_affiliate]
Dear GoodTherapy.org,
I am under 18 and live with my dad and stepmom. I’ve been cutting for almost a year from depression and anxiety and basically not feeling like I want to be here. I HATE the idea of seeing a therapist and “talking about my feelings,” but apparently the school counselor told my dad I needed to see someone outside the school for help. The school counselor doesn’t know about the cutting, but I’ve talked to him a bit because apparently I have “anger issues.”
[fat_widget_right]
So now my dad and stepmother are looking up therapists for me to go see. I really don’t want to talk to anyone about my “issues,” but it’s getting hard to cover the marks on my arms and legs and I don’t know how to stop cutting. And also I know they’re just going to keep me in therapy longer if I refuse to talk. But I REALLY don’t want my parents to know about me cutting myself or the suicidal thoughts I sometimes have. Can I get through counseling without my parents finding out about it? How much is the counselor going to tell my parents about what I say in therapy? —Under Rage
Dear Under Rage,
These are good questions to ask any therapist you see. Find out from them what their policies are regarding confidentiality with people in therapy under 18. Much of what they say will depend on legal and ethical guidelines based on where they live and what kind of license they have. When I work with people under the age of 18, I discuss in great detail with both the young person and the parents what those guidelines are. That allows everyone to have the same understanding and expectation about how the process works. It also allows the young person to decide how much to share with me and to be aware of what my responsibilities to report are.
Most professionals are obligated to report when a person in therapy, regardless of age, is in imminent danger. That danger could be significant risk of suicide or conditions of abuse/neglect. Thoughts of suicide alone, however, do not necessarily trigger a mandated report—it depends on the circumstances. There are many people who have such thoughts but no intention or plan on following through. What is essential, however, is that anyone who is struggling with thoughts of suicide finds sources of support with whom they can talk. A trusted therapist is a great option. There are also national hotlines where you can reach out for support 24/7.
I hear the frustration in your message about all that the adults in your world “apparently†believe to be true for you. Instead, look at what YOU can get out of this experience. You can have a voice and share your truth with someone.
I’ve worked with a number of people who also HATED the idea of talking about their feelings. Usually that stems from a place of fearing they would be judged, a massive discomfort with feeling vulnerable and exposed, and a reluctance to trust someone they don’t know well. All of those feelings are natural. I can share with you that all of those people, in their own time, came to trust me and the process. When you find a therapist you can work with, who allows you to share at your own pace, who offers you a safe place to speak your truth without fear of being judged, counseling can be an amazing experience.
If I can offer you a suggestion, don’t reject therapy completely because it feels like something being “done†to you. I hear the frustration in your message about all that the adults in your world “apparently†believe to be true for you. Instead, look at what YOU can get out of this experience. You can have a voice and share your truth with someone. You can get support for the anger, anxiety, and depression you say you’ve been feeling for a year now. You can have support in finding alternative strategies beyond cutting to cope with the intensity of the feelings you have. You can be seen. You can be heard.
Nobody can make you share what you aren’t willing to share. You are right, though, that refusing to talk or engage will likely limit your choices and your control over your situation. So, how can you engage in ways that work for you? Ask your potential therapist the tough questions about confidentiality and how they manage those issues. Find out if your parents are willing to let you take part in the process of choosing a therapist. Many professionals have directory profiles and websites that can tell you a bit about what they might be like to work with. I’ve had people meet me first before deciding to work with me. Many therapists are very willing to meet to assess fit, as we know a good fit leads to more positive outcomes. You might just find someone you can open up to who can offer relief from what you’ve been feeling.
Best of luck,
Erika
 Editor’s note: This article contains mentions of suicide. Details have been altered to protect client privacy.
Editor’s note: This article contains mentions of suicide. Details have been altered to protect client privacy.
Bill promised not to kill himself, as long as he could continue to see me. Despite his severe depression, this 67-year-old Vietnam veteran showed up at my office each week at 1 p.m. on Tuesday wearing the same stained beige t-shirt, torn jeans, and a faded baseball cap with the words United States Air Force embroidered boldly across it. His sour body odor choked the room as I listened to the horror of his nightmares and gauged the degree to which he wanted to kill himself that day. The hour before he arrived, I spent readying myself for his whirlpool of despair and avoiding the obvious fact that this person wasn’t getting better. In my 20 years as a psychotherapist, I had never encountered someone in therapy who worried me as much as Bill.
I was his third therapist. Before he reached me, Bill had already spent years in weekly therapy at our facility. His previous therapist ended treatment because he believed Bill was “not interested in getting better.†Still, I was optimistic that I could help this stubborn, but fragile, man. Bill reinforced my aspirations at first by leaving our sessions lighter. His depression soon reappeared, however, like a disturbed old friend who comes for a visit, somehow moves in, and requires a police escort to leave. But no matter how depressed Bill felt, he would always make it a point to end our sessions with, “I really appreciate our work together, and thank you for your time.†This gave me hope.
[fat_widget_right]Bill was angry, bitter, and resentful about many things. At the top of his list was his sister, Kate. What likely started as sibling rivalry in childhood simmered into a putrid sludge of jealousy, betrayal, and abandonment so thick that Bill’s irritable bowel syndrome flared up whenever his sister’s number flashed across his cell phone. Unfortunately, Kate was the only other consistent person in Bill’s life.
The only way I seemed to get through Bill’s anger was to connect with him as a person, not as a therapist. Whenever I strayed from my clinical persona and mentioned that I enjoyed a certain book or movie, he came alive. Bill would recommend certain books or DVDs and loan them to me like a devoted uncle. These exchanges touched my heart and showed me the thoughtful and caring man below his embittered exterior.
Over the first four years of our work, I came to recognize that Bill might be getting worse. There were ups and downs, but the downs came more quickly and stayed longer. His melancholy started to weigh me down, too. I began to feel burdened by our sessions and had trouble tolerating his misery. I knew it was my professional responsibility to work through my resistance, but I struggled. At times, his pain was almost too much to bear.
Somewhere around the middle of his fifth year of treatment, Bill blurted out that he found a “foolproof†suicide method on the Internet. His eyes twinkled as he shared that the suicide would mimic some other form of death.
Somewhere around the middle of his fifth year of treatment, Bill blurted out that he found a “foolproof†suicide method on the Internet. His eyes twinkled as he shared that the suicide would mimic some other form of death. “No one would ever know,†he mouthed his excitement. His demeanor frightened me so much I changed the subject. Later, once we had both calmed down, I asked him to tell me more about this method, but he had moved on. “I don’t want to talk about it,†he insisted. So, I assessed him once again for suicide risk. No, he reminded me, he wouldn’t kill himself as long as he could continue to see me.
After that, I started to question whether I’d be able to keep Bill alive. The gravity of my increasingly impossible duty sat on top of me in session, as I drove home, and at night while in bed. I felt so powerless. The truth was, I couldn’t secure Bill’s safety unless he verbalized intent to kill himself—only then could I hospitalize him. Bill knew this. He knew exactly what words would have him locked up in the psych ward, and he carefully avoided them. He had been hospitalized once before, a number of years ago, and wished never to return.
A few months later, Bill came to session particularly upset. He was being evicted from his flat where he’d lived for the past 30 years. His landlords had sold the property. Bill decided he was going to fight it. His determination seemed to embolden both of us for a few weeks. Bill secured a lawyer and showed up to session bathed and wearing clean clothes. I began to believe that if we could win this fight we might finally lift his depression. As it became clearer that Bill would be forced to leave, I changed course. Not Bill, though.
Bill started missing sessions. At first, I was secretly relieved that I didn’t have to spend the hour arguing with him about finding a new place to live. These disputes wore me out. But I was also worried about him, so after a couple of cancelled appointments I insisted he come back in. Things were not going well at all. Eviction was imminent. As a last resort, Bill had called his sister to ask if he could “crash†for a couple of weeks. Kate refused.
Bill sobbed in my office. I felt crushed, too, as I assessed for suicide and he promised, as always, not to hurt himself. His mood improved as we talked over his situation, and he felt supported. Toward the end of session, he promised to see a doctor about his IBS and attend a stress management group before our next meeting.
When I arrived at work the following Tuesday, I had a voicemail waiting for me from the site manager of our clinic. Bill’s sister, Kate, had contacted him. She hadn’t heard from Bill on her 40th anniversary and found this strange. Nor was he answering his phone. Kate decided to call the police to check Bill’s apartment, where they found him found him on the bathroom floor, dead. The message ended by informing me Bill’s body would be sent for an autopsy to rule out suicide.
I cherished Bill and felt honored by his trust. Then I remembered the words he had used about a year ago—“foolproof suicide.†My grief turned to panic as I began to question whether he killed himself or not, and if so, could I have prevented it?
I locked the door to my office, put my head on my desk, and wept. I was devastated. I cherished Bill and felt honored by his trust. Then I remembered the words he had used about a year ago—“foolproof suicide.†My grief turned to panic as I began to question whether he killed himself or not, and if so, could I have prevented it? Why hadn’t I pressed him more for details? My thoughts jumped down that dark black hole, until I remembered I could only take Bill at his word. He had promised not to kill himself that day, as well as the gazillion other days I had asked him.
The coroner’s report came back a month later. It determined the cause of death to be a myocardial infarction—heart attack. I was relieved. Bill’s death was due to natural causes. But to this day, I still wonder if he may have used the “foolproof suicide†plan. He had come to the end of his road: he was elderly, physically impaired, soon to be homeless, and completely alone. His last remaining pleasure might have been to make sure he would ruin his sister’s anniversary each year by dying on the same day. Yet I can’t be fully certain. If he had taken any actions to bring about his death, they left no trace.
Bill’s death had me asking some very painful questions. Was there more I could have done? Was the therapy unsuccessful? And, most damning—was I to blame for his demise? Thankfully, the uncertainty around his death left many of these questions unanswerable and spared me from the agony I would have felt had I known for certain that he committed suicide under my care. In the end, after I tried so hard to protect Bill, he in his death may have, in fact, protected me. I will never know for sure, and I’m pretty certain that Bill intended it that way.
Susan Oren is a clinical psychologist who has been treating clients and training psychology pre-doctoral interns for over 25 years. Her writing has appeared in professional journals and books as well as in the Huffington Post and three anthologies.
 More than a quarter of Americans experience mental health issues each year, and the World Health Organization reports that depression is the leading cause of disability worldwide. However, many Americans think mental health care is both expensive and difficult to access, according to a study jointly sponsored by the National Action Alliance for Suicide Prevention, the Anxiety and Depression Association of America, and the American Foundation for Suicide Prevention.
More than a quarter of Americans experience mental health issues each year, and the World Health Organization reports that depression is the leading cause of disability worldwide. However, many Americans think mental health care is both expensive and difficult to access, according to a study jointly sponsored by the National Action Alliance for Suicide Prevention, the Anxiety and Depression Association of America, and the American Foundation for Suicide Prevention.
In a survey of 2,000 adults, most (almost 90%) said they equally valued physical and mental health. One third reported that mental health care is hard to access, and 40% said high costs are a barrier to treatment. Forty-seven percent thought they had experienced a mental health issue, but only 38% of them had received treatment.
[fat_widget_right]Among those who sought treatment, therapy was the most popular option, with 82% pursuing psychotherapy and 78% taking medication. Eighty-six percent said that they knew mental health conditions such as depression increase the risk for suicide, but only 47% knew that anxiety-related conditions could also increase one’s suicide risk.
Though federal laws mandate equal coverage for mental and physical health, a number of recent reports suggest that many insurers continue to deny mental health claims.
64% of Psychology Experiments Fail Replication Test
In May, GoodTherapy.org reported on research suggesting that the majority of psychology studies could not be reproduced by subsequent researchers. Reproducibility is a hallmark of sound science. When a study’s results cannot be recreated, this suggests that the study could have been flawed, biased, or a fluke. Now, the results of that research have been published in Science, sparking debates about a so-called crisis in psychology. The research argues that the results of only a quarter of social psychology experiments and half of cognitive psychology experiments could subsequently be reproduced.
Living Small: The Psychology of Tiny Houses
Tiny houses are trending all over social media. For young people facing an expensive housing market, more economically sized homes can be enticing. These houses encourage people to reduce their carbon footprint by living simply, offer greater mobility because they can easily be moved by a trailer, and are much more affordable than standard-size homes. Moving into a tiny home may require significant downsizing of clothing, furniture, and belongings, but the advantages may include increased control over one’s housing experience, a private alternative to keeping costs down, and the ability to personalize design to fit one’s mood.
 Health Buzz: Alcohol Education Should Begin at Age 9
Health Buzz: Alcohol Education Should Begin at Age 9
Parents often delay talking to their kids about alcohol until the adolescent years, but a new survey published in the American Academy of Pediatrics suggests that these conversations should begin much earlier. The survey found that two thirds of teens had consumed alcohol by their high school graduation and that a quarter have had more than just a few sips before eighth grade. Researchers also found that children and teens drink more heavily than adults, raising concerns about alcohol poisoning and addiction. To give kids accurate and relevant information, the report recommends parents begin the alcohol conversation by the time their children are 9 years old.
Religion Rarely Part of ICU Conversation
Though three quarters of people charged with making health care decisions in an intensive care unit report that religion and spirituality are “fairly†or “very†important in their lives, less than 20% of family health care meetings involve discussion of religion or spirituality with doctors and other caregivers. Particularly when discussing end-of-life decisions, religion can be important, but it is usually the caregiver, not the doctor, who broaches the subject.
Japan’s Worst Day for Teen Suicides
September is National Suicide Prevention Month. For many Japanese parents, it may also be a time of increased concern about suicide among their teens. In Japan, more school students commit suicide on September 1 each year than on any other day. Though experts have posited various explanations—such as worries regarding bullying at school after a summer break free of emotional and physical attacks from peers—suicide remains common. Japan has one of the world’s highest suicide rates, and suicide is the leading cause of death among people aged 15 to 39. Figures from the Japanese government show that more than 18,000 adolescents under the age of 18 committed suicide between 1972 and 2013.
Oliver Sacks, Renowned Neurologist Who Wrote About His Cancer, Dies at 82
Famed author and neurologist Oliver Sacks died of cancer at his home on Sunday, August 30. Sacks wrote about unusual neurological conditions, often naming books after symptoms he saw in his clinical practice, such as The Man Who Mistook His Wife for a Hat. He was the inspiration for the doctor played by Robin Williams in the 1990 movie Awakenings, which is based on Sacks’ 1973 book of the same name.
Lack of Sleep Puts You at Higher Risk for Colds, First Experimental Study Finds
 According to a study of 164 healthy people, inadequate sleep could increase the risk of developing a cold. Scientists monitored participants’ sleep patterns for a week, then quarantined them in a hotel for five days and exposed them to a cold virus. Researchers also checked the participants’ blood for an antibody that fights the common cold, then removed participants who had the antibody to make sure those participants would not bias the infection rates of the group.
According to a study of 164 healthy people, inadequate sleep could increase the risk of developing a cold. Scientists monitored participants’ sleep patterns for a week, then quarantined them in a hotel for five days and exposed them to a cold virus. Researchers also checked the participants’ blood for an antibody that fights the common cold, then removed participants who had the antibody to make sure those participants would not bias the infection rates of the group.
At the end of the quarantine period, 45.2% of those who slept less than five hours a night exhibited at least one sign of illness—revolving around mucus production—and one other immune response. Of those who slept five to six hours, the cold rate was 30%, compared to 22.7% for those who slept six to seven hours. The rate was only 17.2% for those who got more than seven hours of sleep. At the end of the study, researchers determined that people who slept less than five hours per night were 4.5 times more likely to get sick than those who slept seven hours or more.
 “Self-injury is an expression of acute psychological distress. It is an act done to oneself, by oneself, with the intention of helping oneself rather than killing oneself. Paradoxically, damage is done to the body in an attempt to preserve the integrity of the mind.†—Sutton and Martinson, 2003
“Self-injury is an expression of acute psychological distress. It is an act done to oneself, by oneself, with the intention of helping oneself rather than killing oneself. Paradoxically, damage is done to the body in an attempt to preserve the integrity of the mind.†—Sutton and Martinson, 2003
Self-injury is a serious phenomenon that affects millions of adolescents. Current prevalence estimates of non-suicidal self-injury (NSSI) among middle school and high school students range from 15% to 20%, and some studies estimate rates even higher than that.
It can be difficult for family members, friends, and even professionals to understand what causes young people to hurt themselves, or to know how to respond. Discovering that a child or adolescent is engaging in self-harming behaviors can be frightening. It is not uncommon to feel panic, worry, or even disgust when you suspect or discover this type of behavior. Having accurate information is an important first step for parents, teachers, and other helping professionals who may be the first line of defense when adolescents engage in non-suicidal self-injury.
What’s the Difference Between Self-Injury and a Suicide Attempt?
[fat_widget_right]
Non-suicidal self-injury (NSSI) describes the intentional injury to or destruction of one’s own body tissue, most commonly through cutting, burning, or self-hitting. Sometimes parents wonder if cutting and other self-harming behaviors are simply a cry for attention. If that’s true and someone needs attention that badly, then I can’t imagine a more appropriate response than to give it. Instead of looking at it as a bid for attention, though, try thinking of it as an attempt at communication.
Cutting and other forms of self-harm should always be taken seriously. Most individuals who engage in non-suicidal self-injury do so in secret and go to great lengths to hide the behavior from others. Most often, NSSI is performed as a way to regulate or modulate strong, painful emotions. Sometimes, NSSI is also described as a way for individuals who feel numb to “feel alive.â€
NSSI should not be construed as a failed suicide attempt. NSSI is an attempt to live with or manage painful feelings—unlike suicide, which attempts to permanently end pain by ending one’s life.
NSSI should not be construed as a failed suicide attempt. NSSI is an attempt to live with or manage painful feelings—unlike suicide, which attempts to permanently end pain by ending one’s life. It is important to note, however, that although they serve different functions, NSSI is associated with an increased risk of future suicide attempts, and therefore should never be taken lightly.
Signs to Watch For
It is important for parents, teachers, and other helping professionals to learn to recognize the signs and symptoms of self-injury. A few things to watch for include: wearing long sleeves even when it is hot outside; a pressing desire for a lot of time alone; and, of course, unexplained, or suspicious cuts, burns, or bruises.
Sometimes, individuals who engage in self-harming behaviors may appear to be clumsy or have frequent accidents, and use these incidents to explain self-inflicted injuries. Adolescents who experience depression or anxiety, have difficulty solving problems, or who tend to feel things deeply may have an increased risk of turning to NSSI as a method of coping.
What to Do If Your Child Is Cutting
How you respond matters! If you suspect or discover that your child is cutting or engaging in other self-harming behaviors, it is important to seek help from a qualified mental health professional. A professional will begin with an assessment and may recommend family or individual therapy, or a combination of both.
Early intervention is best, so don’t wait to get help. Treatment can be effective at both reducing the behaviors and addressing painful emotions.
Reference:
Sutton, J., & Martinson, D. (2003). Because I hurt: Understanding self-injury & healing the hurt. Oxford: How To Books.